
Physical Causes Of Reduced Sensitivity
Reduced penile sensitivity (RPS) has a number of causes, but the causes break down into two major categories: nerve damage and circulatory problems.
Interestingly enough, ED and reduced penile sensitivity have causes which can usually be attributed to the same broad categories, and indeed, some level of RPS and ED may occur together.
Reduced penile sensitivity is uniquely a problem of nerve damage or desensitizing the nerves in the penis.
This discussion really relates to permanent nerve damage, not desensitized nerves for reasons such as excessive stimulation or cold temperatures.
Nerve damage can occur in the penis itself from causes such as trauma directly to the penis, or from damage caused by removing part of the penis, as in circumcision.
Studies have generally indicated that ED and delayed ejaculation are increased in men with circumcised penises. (Additional detail can be found at the Circumcision and Information Pages, www.cirp.org)
Damage can also occur in the nerves in the groin area which lead into the penis, around the prostate gland, particularly in prostatectomy surgery, and in injuries to the back, especially around the S-4 vertebra.
Nerves to the penis pass from the spine, under the groin area between the anus and testicles (the perineum).
Trauma in that area, even bicycle riding on a seat which applies excessive pressure, can cause damage to those nerves and so lead to a loss of penile sensitivity.
Severe vascular disease can also decrease the sensitivity of penile nerves, but usually vascular problems have a greater impact on the ability to get an erection (ED).
Some diseases, such as diabetes may affect both vascular integrity and function of nerves.
It is the opinion of this author that the majority of penile sensitivity issues are caused by neural damage primarily due to circumcision, which by its definition removes an integral part of the penis.
The foreskin is not “just skin”, but includes an inner foreskin of special kind of tissue with (1) a density of soft-touch erogenous nerves found nowhere else in the male body, (2) smooth mucosa cells which secrete various immunological secretions (3) apocrine glands secreting feromones.
(For a detailed list of foreskin functions, go to the website www.the-penis.com) The inner foreskin in an adult intact male is about 7.5 square inches (1.5 by 5 inches circumference).
A circumcision therefore crushes and destroys 50-90% of the nerve endings which lend pleasure to sex.
Yet it was not until the late 1990s that anyone decided to study the foreskin in detail, and it was the accepted theory that circumcision did not damage the penis or reduce sensitivity. (The studies are explored in the next section.)
For most men, the reduction of sensitivity goes unnoticed until poor circulation or decreased hormone levels aggravate the condition.
Since most circumcisions are done neonatally within 2 days of birth, there is no basis of comparison for intact verses circumcised sensitivity.
Studies and knowledgebase information relating to reduced sensitivity
This section reviews six significant published medical studies of penile sensitivity, published mainly in the 1990 and 2000 decades.
These studies have come up with two answers about penile sensitivity relating to circumcision (1) that circumcision does not affect penile sensitivity, and (2) that circumcision does significantly affect penile sensitivity.
Interestingly, both answers are correct – it depends on what the studies measured, and where on the penis the measurements were made. Studies which focus exclusively on the glans suggest no effect. Studies which include the foreskin show significant losses.
These studies are briefly discussed below.
- Masters and Johnson, 1964
- Taylor-inner foreskin, 1996
- Taylor-ridged bands, 1999
- Fink, 2001
- Bleustein, 2005
- Sorrells, 2006
Review of the intact penis anatomy
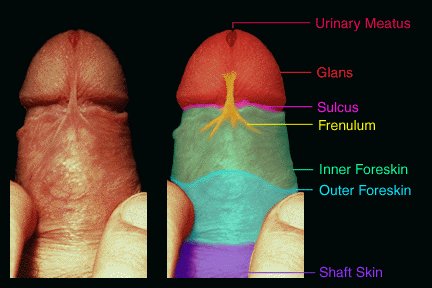
In order to understand the studies, it is instructive to discuss the anatomy of the intact (uncircumcised) penis, and show the foreskin segments which are amputated in a circumcision. The drawings below show the penis with retracted foreskin, viewed from the top and bottom.
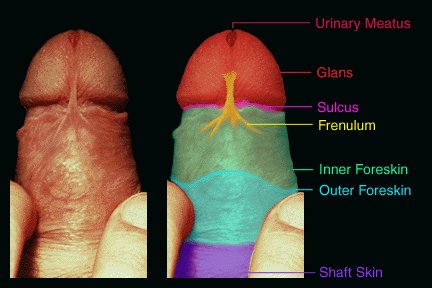
 Penis") 1 Glans
1 Glans
2 Sulcus
3 Muco-cutaneous junction
4 Inner foreskin – ridged bands
5 Frenulum at muco-cutaneous junction
6 Outer foreskin
7 Shaft skin
When the intact penis is flaccid, the foreskin is pulled forward by the frenulum to cover the glans.

During an erection, the foreskin will normally slide back enough to expose or partially expose the glans with sufficient slack to allow the foreskin “tube” to slide.
During sexual activity, the intact foreskin slides back and forth against the glans, providing erogenous neural responses from the extremely sensitive ridged bands of the inner foreskin.
Contrary to old wisdom, the glans is not very sensitive. As will be discussed in this section, the ridged bands and frenulum of the inner foreskin have extremely sensitive light-touch tactile nerve endings.
Additionally, there are pressure-sensitive nerves internally at the tip of the penis beneath the glans, which are believed to have a part in the ejaculation response.
Most circumcised men admit to a “sweet spot”, typically just below the “V” of the glans on the underside of the penis, or sometimes an area just below the sulcus. These small areas of sensitivity are in fact the remnants of their original foreskins.
Video – the sensitive part of the penis
In circumcision, the tissue from the sulcus to the junction with the shaft skin is removed. The procedure is usually performed on the folded foreskin (not retracted) typically by cutting the foreskin at both ends and suturing the ends together.
In the case of “medical” neonatal circumcisions, the foreskin (bonded to the glans in infants) is torn from the glans, cut with a slice from the tip to the corona of the glans, and a clamp slid under and over the now loose foreskin, which is screwed tight to crush the foreskin.
All of the tissue from the glans to the junction with the shaft skin is therefore destroyed. Neo-natal circumcisions are usually more extreme than adult circumcisions, since the fully positioned clamps leave little or no inner foreskin from the glans.
The following studies chronicle the understanding of the functions and arousal of the penis during sex, in roughly chronological order.
Masters and Johnson, Human Sexual Response, Published 1966, Little, Brown & Company: “No clinically significant difference could be established between the circumcised and the uncircumcised glans during these examinations.”
As a part of their comprehensive book on male sexuality, Masters and Johnson included short synopsis wherein they describe a study of comparative sensitivity of circumcised and non-circumcised men based mainly on the glans. The study itself was never published, and the methods and controls of the study were never subject to peer scrutiny.
The study focused mainly on the circumcised population, and on the glans as an area of penile sensitivity.
The authors noticed but failed to grasp the significance of different masturbation techniques in intact and circumcised men, which would have held a clue that the foreskin has sensitive nerves not found elsewhere in the penis.
In a section discussing “automanipulation”, that is masturbation, they stated: “Uncircumcised males have not been observed to concentrate specifically on the glans area of the penis. Normally they follow the usual pattern of confining manipulative activity entirely to the penile shaft. Stroking techniques rarely move sufficiently distal on the shaft of the penis to encounter more than the coronal ridge of the glans even late in plateau phase just before ejaculation”.
Taylor et al: Specialized mucosa of the penis and its loss to circumcision, British Journal of Urology, Volume 77, February 1996: “We postulate that the ‘ridged band’ with its unique structure, tactile corpuscles and other nerves, is primarily sensory tissue and that it cooperates with other components of the prepuce.”
This was the first in-depth study which investigated the anatomy of the prepuce (foreskin), and from that investigation postulated the role which the foreskin plays in the functioning of the penis, and penile sensitivity. The foreskin anatomy was studied with samples taken from deceased males. They reported:
“Skin and mucosa sufficient to cover the penile shaft was frequently missing from the circumcised penis. Missing tissue included a band of ridged mucosa located at the junction of true penile skin with smooth preputial mucosa. This ridged band contains more Meissner’s corpuscles than does the smooth mucosa and exhibits features of specialized sensory mucosa…Circumcision also ablates junctional mucosa that appears to be an important component of the overall sensory mechanism of the human penis.”
“We postulate that the ‘ridged band’ with its unique structure, tactile corpuscles and other nerves, is primarily sensory tissue and that it cooperates with other components of the prepuce. In this model, the ‘smooth’ mucosa and true skin of the adult prepuce act together to allow the ‘ridged band’ to move from a forward to a ‘deployed’ position on the shaft of the penis. In short, the prepuce should be considered a structural and functional unit made up of more and less specialized parts.”
Cold and Taylor: The prepuce, British Journal of Urology, Volume 83, January 1999: “Excision of normal, erogenous genital tissue from healthy male or female children cannot be condoned, as the histology confirms that the external genitalia are specialized sensory tissues.”
This study was really a review of published papers and evaluation of the knowledge base on genital anatomy and penile sensitivity, particularly with respect to the prepuce, for both males (the male foreskin) and for the comparative structures in females (the female prepuce is the clitoral hood).
The review clearly indicates that the ridged bands and frenulum of the inner foreskin to be the most sensitive erogenous tissue of the penis, and the glans itself to be relatively insensitive.
“The prepuce is a common anatomical structure of the male and female external genitalia of all human and non-human primates; it has been present in primates for at least 65 million years, and is likely to be over 100 million years old, based on its commonality as an anatomical feature in mammals.”…
“The prepuce is primary, erogenous tissue necessary for normal sexual function. The complex interaction between the protopathic sensitivity of the corpuscular receptor-deficient glans penis and the corpuscular receptor-rich ridged band of the male prepuce is required for normal copulatory behaviour.”…
“Surgical amputation of the prepuce removes many of the fine-touch corpuscular receptors from the penis and clitoris. In males, circumcision is essentially a partial penile mucosectomy…”
“Excision of normal, erogenous genital tissue from healthy male or female children cannot be condoned, as the histology confirms that the external genitalia are specialized sensory tissues.”
Fink et al, Adult circumcision outcomes study: effect on erectile function, penile sensitivity, sexual activity and satisfaction, Journal of Urology, v167(5), 2001: “We found that circumcised men were instead more likely to have erectile dysfunction…”We found a statistically significant decrease in penile sensation following circumcision in men but our respondents had mixed feelings.”
This study consisted of a survey, questionnaire and follow-up discussions for a group of men, who were circumcised as adults for a medical condition or for personal reasons preferred to be circumcised. It was rather unique, as it looked at before and after conditions to assess perceived changes by these men.
“We found that circumcised men were instead more likely to have erectile dysfunction. Our study populations differ in that we evaluated men circumcised as adults but the worsened erectile function remained when adjusted for age and the presence of diabetes, depression and cardiovascular disease.”…
“We found a statistically significant decrease in penile sensation following circumcision in men but our respondents had mixed feelings. Some responders appeared to be better able to satisfy their partners after circumcision but some men were not satisfied with the decreased sensation of physical stimulation. It seems that sexual pleasure means different things to different men and should be more specifically defined in future studies.”…
Bleustein et al., Effects of Circumcision on Male Penile Sensitivity, Paper read at the American Urological Association 98th Annual Meeting at Chicago Illinois, 2003: “We demonstrated that there are no significant differences in penile sensation between circumcised and uncircumcised men with respect to vibration, spatial perception, pressure, warm and cold thermal thresholds in both patients with and without erectile dysfunction.” [ based on measurements of the glans penis –ed.]
This study attempted to establish the penile sensitivity difference between circumcised and non-circumcised adult men. The study tested different sensory thresholds on the dorsal midline glans of the penis.
For intact (uncircumcised) men, the foreskin was retracted and held back behind the glans to allow equal tests on the glans of both circumcised and uncircumcised men. The results showed no significant difference between the two groups at the glans penis; the inner foreskin of intact men was retracted and excluded from the study.
“Patients were subsequently tested on the dorsal midline glans of the penis. In uncircumcised males, the foreskin was retracted for testing. Vibration (Biothesiometer), pressure (Semmes-Weinstein monofilaments), spatial perception (Tactile Circumferential Discriminator), and warm and cold thermal thresholds (Physitemp NTE-2) were measured.”
“We present a comparative analysis between uncircumcised and circumcised men using a battery of quantitative somatosensory tests that evaluate the spectrum of small to large axon nerve fibers. We demonstrated that there are no significant differences in penile sensation between circumcised and uncircumcised men with respect to vibration, spatial perception, pressure, warm and cold thermal thresholds in both patients with and without erectile dysfunction.” [as measured on the glans penis – Ed.]
Sorrells et al.: Fine-touch pressure thresholds in the adult penis, British Journal of Urology International (BJUI), V99(4), April, 2007: “The glans of the circumcised penis is less sensitive to fine touch than the glans of the uncircumcised penis. The transitional region from the external to the internal prepuce is the most sensitive region of the uncircumcised penis and more sensitive than the most sensitive region of the circumcised penis. Circumcision ablates the most sensitive parts of the penis.”
This study was a landmark study because for the first time it measured fine-touch sensitivity of all areas of the intact and circumcised penis, rather than just the glans, which was found to be significantly lower in sensitivity than other parts of the organ. The results clearly showed that any future sensitivity studies must include the entire penis.
[The objective of this study was] “To map the fine-touch pressure thresholds of the adult penis in circumcised and uncircumcised men, and to compare the two populations.”…”When compared with the most sensitive area of the circumcised penis, several locations on the uncircumcised penis, which are missing from the circumcised penis, were significantly more sensitive.”
“Despite the controversy over the long-term impact of male circumcision, no thorough, objective, quantitative studies measuring the long-term sensory consequences of infant circumcision have hitherto been reported. The present study provides the first extensive mapping of the fine-touch pressure thresholds of the adult penis…”